Managed care plans recognize CRNAs for providing high-quality anesthesia care with reduced expense to patients and insurance companies. The cost-efficiency of CRNAs helps control escalating healthcare costs.
The Continued Professional Certification (CPC) Program, which replaced the former recertification program, focuses on lifelong learning and is based on eight-year periods comprised of two four-year cycles. Each four-year cycle has a set of components that include:
- 60 Class A credits (assessed continuing education)
- 40 Class B credits (professional activities)
- Four Core Modules (current literature and evidence-based knowledge; also count as Class A credits)
- A 2-year Check-in at the midpoint of each four-year cycle
- Confirm current state licensure and attest to engagement in anesthesia practice, and
The CPC Assessment component is only required in the second 4-year cycle and can be taken during any testing windows in that second cycle. For complete information on all components of the CPC Program, click the button below.

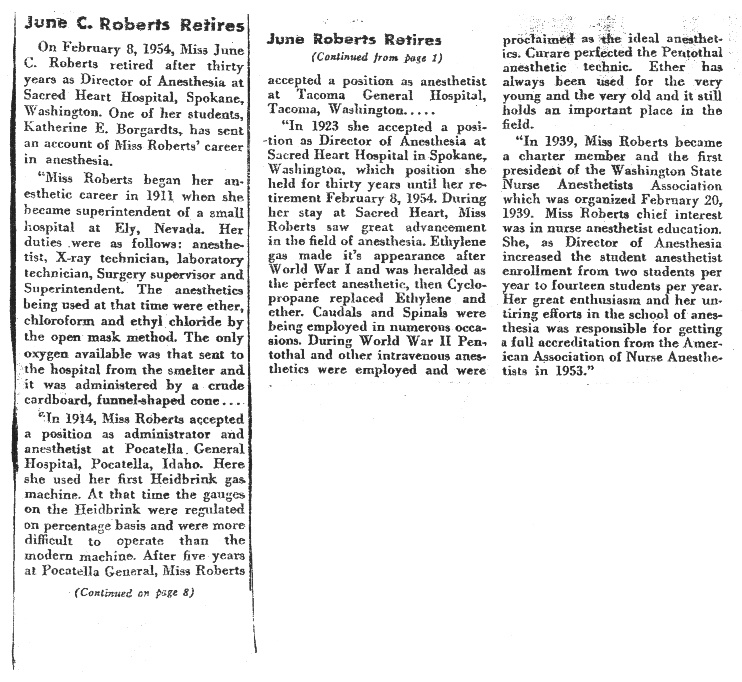
In the Spring of 1936, Spokane hospital representatives Elizabeth Scully, June Roberts, Alice Claude and Mary Leonard met at a luncheon in the Davenport Hotel. Their purpose was to form plans for the creation of an association for Nurse Anesthetists.
A few short years later, on 20 February 1939, the Washington Association of Nurse Anesthetists (WANA) was organized. Their first meeting occurred at the Davenport Hotel in May 1940.
June Roberts was a charter member and first president of WANA. Her primary interest was to promote and encourage nurse anesthetist education. During her time as president of WANA, she increased anesthetist enrollment from two students per year to fourteen. June’s enthusiasm and assiduous efforts in the school of anesthesia was responsible for obtaining full accreditation from the American Association of Nurse Anesthetists in 1953. The following year, she retired after three decades as Director of Anesthesia at Sacred Heart Hospital in Spokane.